Eπείγουσα Νοσηλευτική και εκπαίδευση ασθενών
Η εκπαίδευση των ασθενών είναι το κλειδί για τη διαχείριση των πιο λογικών και χρονικών συνθηκών. Ο σκοπός αυτού του άρθρου είναι να εξερευνήσει και να αναλύσει των τύπο των παρεμβάσεων και των αποτελεσμάτων που χρησιμοποιούνται σε αυτό το περιβάλλον και να κάνει σαφές αν υπάρχουν επείγοντα στοιχεία αποτελεσματικότητας αυτών των παρεμβάσεων.
Abstract
PATIENT
COUNSELING and education are key components for effective
self-management and monitoring required with many acute and chronic
conditions. Current evidence-based guidelines for complex conditions,
such as asthma and diabetes, include patient education as an expected
aspect of care (Canadian Asthma Consensus Group, 1999; Taskforce on Community Preventative Services, 2002).
Patient education is provided in a variety of settings across the
continuum of care. In ambulatory care and outpatient settings, health
education has been shown to improve outcomes for patients (Deakin, McShane, Cade, & Williams, 2005; Gibson et al., 2007).
Although not always recognized, emergency departments (EDs) offer an
important opportunity for educational interventions. However, on the
basis of studies utilizing chart audit and patient recall, the ED
appears to be underutilized as a setting for delivery of health
education (Demorest, Posner, Osterhoudt, & Henretig, 2004; Dunn et al., 1993).
EDs
have become major access points for healthcare in many jurisdictions,
where a large proportion of visits are for nonurgent problems (Canadian Institute for Health Information, 2006). In part, presentation to the ED for nonurgent conditions is due to poor access to primary care (Drummond, 2002) and for some, it may be the only point of contact with the healthcare system (Partridge, Latouche, Trako, & Thurston, 1997).
Because of this shift in healthcare utilization, there is an increasing
need to consider delivery of patient education and counseling in EDs.
However, there are many barriers to providing adequate patient education
in this setting. Overcrowded conditions and the length of time required
to provide the necessary information may affect ED staffs' ability to
provide teaching (Drummond, 2002). While some believe that the ED is not an appropriate venue for education (Masters, Hall, Phillips, & Boldy, 2001),
others believe that it offers a unique "teachable moment" during which
time patients may be motivated to learn from healthcare providers (Bowling, 1993; Todd, 1996).
In some cases, moderate stress enhances an individual's ability to
learn, particularly if the information provided is not too complex (Shors, 2004). Considering all
opportunities for patient counseling and self-management support
including the ED seems prudent in today's healthcare environment.
Bloom's Taxonomy of Learning Domains is a widely used framework in education that identifies learning outcomes or domains (Redman, 1988).
According to Bloom's theory, learning can be divided into three main
domains: cognitive, affective, and psychomotor. Each domain includes
levels of increasing mastery. Cognitive learning
involves the acquisition of knowledge. Simple cognitive goals can be
measured by evaluation of recall, understanding, or comprehension,
whereas more complex goals may measure the application of knowledge or
development of a model or framework. Affective learning
involves the internalizing of values, attitudes, or beliefs. In its
simplest form, affective learning goals can include being willing to
hear information or actively participating in learning. Complex learning
goals in the affective domain require the participant to adopt a new
value or belief system. The psychomotor domain
is a learning process that involves the mastery of skills. These
learning goals can range from simply copying a demonstration to
automated mastery of the technique. Weston and Cranton (1986) utilized Bloom's taxonomy and identified optimal teaching methods for each level of the three domains (Table 1).
Although Weston and Cranton's framework was created for use in the
design and evaluation of education in traditional classroom settings and
not healthcare settings, some of the methods suggested may be useful in
the ED. The challenge is to effectively provide the optimal education
using the time and resources available in a setting such as the ED.
 | Table 1. Cognitive, affective, and psychomotor domains |
Currently, we know little about the effectiveness of providing education in the ED. In a 2000 review, Wei and Camargo (2000)
synthesized the research on patient education in the ED identifying
studies related to populations with asthma, myocardial infarction,
psychiatric conditions, and injury and trauma. Because so few studies
focused on education done exclusively in the ED (n = 5), the authors included studies with interventions that continued after discharge from the ED (n = 4) as well as interventions conducted in the coronary care unit and acute care wards (n
= 6). The authors concluded that educational interventions in these
settings, including the ED, improved patient outcomes. Although
similarities may exist between the ED and other acute care settings, key
differences across settings may impact on important factors related to
educational effectiveness, such as time available for teaching and the
anxiety of patients. In addition, although ongoing counseling and
education is ideal, encouraging patients to attend education sessions
may be challenging. In a study evaluating an asthma education program,
only 31% of the 164 eligible participants recruited from the ED attended
the program (Yoon, McKenzie, Miles, & Bauman, 1991).
If individuals are not utilizing primary care for follow-up, it is
important that we understand what can reasonably be delivered in the ED
and determine the effectiveness of interventions provided only during
the ED visit.
METHODS
An explicit search strategy, as well as retrieval procedures and appraisal process, was undertaken with this systematic review. Table 2
provides details of the data sources, search strategy, key words, and
limitations used. Articles were included if they were an evaluative
research study (randomized control trials [RCTs], quasi-experimental, or
observational designs) involving an educational intervention delivered
to adult participants (18 years or older) who presented to the ED for
treatment or an adult who was accompanying a minor child, and who were
subsequently discharged home.
 | Table 2. Studies of educational interventions in the emergency: Data sources and search strategies |
RESULTS
The
search strategy yielded 437 potentially relevant unique citations of
which 19 met the inclusion criteria and comprised the final set for this
review (Figure 1). Although many studies included in this review were also present in the Wei and Camargo's (2000) review, there were a number of new ones (n
= 10) and the scope and focus of the new articles were different. Four
other studies that included interventions initiated and largely carried
out in the ED but continued after discharge were also identified. These
studies have been addressed after presentation of the 19 studies
focusing on interventions in the ED only. Synthesis of the 19 articles
from the primary set and the 4 additional articles are summarized in Table 3.
 | Figure 1. Search process and results. |
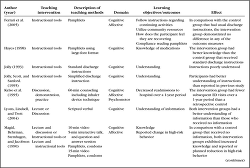
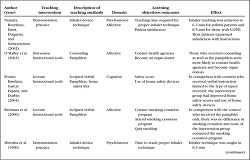
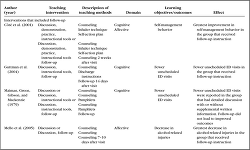
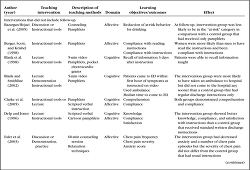 | Table 3. Synthesis of interventions and outcomes in studies of educational interventions in the emergency department (ED) using Bloom's domains |
 | Table 3. Synthesis of interventions and outcomes in studies of educational interventions in the emergency department (ED) using Bloom's domains( |
 | Table 3. Synthesis of interventions and outcomes in studies of educational interventions in the emergency department (ED) using Bloom's domains( |
 | Table 3. Synthesis of interventions and outcomes in studies of educational interventions in the emergency department (ED) using Bloom's domains( |
Type of Educational of Interventions
Many
interventions (15/21) used instructional tools that included provision
of pamphlets, discharge instructions, and/or information sheets. These
instructions were in the form of written or cartoon illustration to be
reviewed by the participant following discharge (Barzargan-Hejazi et al., 2005; Berger et al., 1998; Blank et al., 1998; Blank & Smithline, 2002; Clarke et al., 2005; Delp & Jones, 1996; Ferrari et al., 2005; Hayes, 1998; Jolly, 1993; Jolly et al., 1995; Magid et al., 1990; O'Malley et al., 2003; Posner et al., 2004; Richman et al., 2000). In addition, some interventions also provided supplies for the participants to use, such as condoms (Magid et al., 1990), home safety kits (Posner et al., 2004), or pocket electrocardiograms (Blank et al., 1998).
Although in some cases, the written information was meant to supplement
information provided through other methods such as lecture or
discussion, six studies utilized written-only instruction to identify
the readability and effectiveness of this kind of intervention (Berger et al., 1998; Clarke et al., 2005; Ferrari et al., 2005; Hayes, 1998; Jolly, 1993; Jolly et al., 1995). In some cases, interventions included modified written materials such as instruction in cartoon form (Delp & Jones, 1996), simplified versions of standard discharge instruction (Jolly, 1995), or information in easy-to-read, large-font format (Hayes, 1998).
Some interventions (9/21) involved the use of brief didactic or lecture components to disseminate information (Blank et al., 1998; Blank & Smithline, 2002; Delp & Jones, 1996; Lyons et al., 2004; Magid et al., 1990; Posner et al., 2004; Richman et al., 2000). Lecture is defined as dissemination of information by the healthcare provider while the patient remains passive (Weston, & Cranton, 1986).
For the purpose of this review, interventions were considered to be
lecture if they described the interaction as "scripted," or if the
instruction was done by means of video or audiotape. Of the nine
interventions using lecture, four of the interventions were reported in
three separate studies where video was used as the medium for providing
the lecture (Blank et al., 1998; Blank & Smithline, 2002; Magid et al., 1990). Videos ranged in length from 5 min (Blank et al., 1998; Blank & Smithline, 2002) to 15 min (Magid et al., 1990). Verbal instruction was used in five of the nine lecture interventions (Blank et al., 1998; Delp & Jones, 1996; Lyons et al., 2004; Posner et al., 2004; Richman et al., 2000), and one-on-one instruction was offered to participants in all interventions.
Discussion between provider and the individual was used in 6 of the 21 interventions (Barzargan-Hejazi et al., 2005; Esler et al., 2003; Kelso et al., 1995; Lyons et al., 2004; Magid et al., 1990; O'Malley et al., 2003). Five of the discussion interventions were described as "counseling" (Barzargan-Hejazi et al., 2005; Esler et al., 2003; Kelso et al., 1995; Lyons et al., 2004; O'Malley et al., 2003), and one was in the form of a 5-min question and answer period following a video lecture (Magid et al., 1990). Time required to deliver the counseling intervention was not specified in two studies (Lyons et al., 2004; O'Malley et al., 2003), whereas one discussion intervention was 15 to 20 min in duration (Magid et al., 1990) and the other was 60 min long (Esler et al., 2003).
Demonstration was used in 5 of the 21 interventions and involved a visualization of a skill to be learned (Blank & Smithline, 2002; Esler et al., 2003; Kelso et al., 1995; Numata et al., 2002; Shrestha et al., 1996). Following demonstration, four of the five interventions asked participants to practice the techniques that were taught (Esler et al., 2003; Kelso et al., 1995; Numata et al., 2002; Shrestha et al., 1996).
The demonstration was visual-only or both verbal and visual. Two
interventions used only demonstration and practice to teach proper
inhaler technique (Numata et al., 2002; Shrestha et al., 1996).
Time reported to teach proper inhaler technique ranged from 6.2 to 8.5
min. The remaining studies provided demonstration as part of a larger
intervention. Time to complete these interventions ranged from 5 to 60
min.
Outcomes
Cognitive learning was measured in a number of different ways (Blank et al., 1998; Blank & Smithline, 2002; Clarke et al., 2005; Delp & Jones, 1996; Ferrari et al., 2005; Hayes, 1998; Jolly, 1993; Jolly et al., 1995; Kelso et al., 1995; Lyons et al., 2004; Magid et al., 1990; Posner et al., 2004). Nine of the 12 studies measured basic cognitive domain outcomes including recall of information and comprehension (Blank et al., 1998; Clarke et al., 2005; Delp & Jones, 1996; Hayes, 1998; Jolly, 1993; Jolly et al., 1995; Lyons et al., 2004; Magid et al., 1990; Posner et al., 2004).
These outcomes were evaluated using open-ended interview and knowledge
tests. Four studies measured higher-level cognitive domains such as the
application of information taught (Blank & Smithline, 2002; Ferrari et al., 1998; Kelso et al., 1995; Posner et al., 2004).
Three intervention studies reporting psychomotor outcomes measured
inhaler technique in asthma and/or chronic obstructive pulmonary disease
(COPD) populations (Kelso et al., 1995; Numata et al., 2002; Shrestha et al., 1996). Of the 11 studies reporting affective domain outcomes (Barzargan-Hejazi et al., 2005; Berger et al., 1998; Clarke et al., 2005; Delp & Jones, 1996; Esler et al., 2003; Ferrari et al., 2005; Kelso et al., 1995; Magid et al., 1990; Numata et al., 2002; O'Malley et al., 2003; Richman et al., 2000), three measured change in high-risk behaviors such as drinking (Barzargan-Hejazi et al., 2005), smoking (Richman et al., 2000), and sexual activity or intravenous drug use (Magid et al., 1990).
Each outcome was measured by self-report from participants. One study
measured self-management of asthma as seen by a decrease in hospital
readmissions over a 1-year period (Kelso et al., 1995). Two studies measured satisfaction with instructions (Delp & Jones, 1996; Numata et al., 2002)
reported by participants. In two studies where counseling was provided
to seek advice from other agencies, participants were asked on follow-up
whether they had contacted these agencies (O'Malley et al., 2003; Richman et al., 2000). Four studies measured self-reported compliance with instructions (Berger et al., 1998; Clarke et al., 2005; Delp & Jones, 1996; Ferrari et al., 2005), and one measured use of a home safety kit (Posner et al., 2004).
One study measured change in frequency and severity of symptoms
(noncardiac chest pain) and anxiety scores, pre-and postintervention (Esler et al., 2003).
Effectiveness of Education Interventions in the ED
In
reviewing the 19 studies, a mix of experimental and quasi-experimental
designs were used to evaluate interventions. Ten studies were RCT
designs. On the whole, the trials were well described with detail of the
randomization procedures provided in 8 of the 10 RCTs (Barzargan-Hejazi et al., 2005; Blank & Smithline, 2002; Delp & Jones, 1996; Esler et al., 2003; Ferrari et al., 2005; Hayes, 1998; Numata et al., 2002; Richman et al., 2000) and baseline comparisons between intervention and control groups provided for 9 of the RCTs (Barzargan-Hejazi et al., 2005; Blank & Smithline, 2002; Delp & Jones, 1996; Esler et al., 2003; Ferrari et al., 2005; Hayes, 1998; Magid et al., 1990; Posner et al., 2004; Richman et al., 2000). Nine other studies included cohort and case-controlled designs. Of these studies, three included a control group (Kelso et al., 1995; Lyons et al., 2004; O'Malley et al., 2003) and one included two intervention groups (Lyons et al., 2004).
Of
the 10 RCTs, six reported statistically significant improvements in the
intervention in comparison with the control group, whereas two reported
improvements in some of the learning goals and two found no
improvements. One study that reported significant results did not
describe the control group (Numata et al., 2002),
but the remaining studies all described intervention and control groups
that were similar with respect to baseline characteristics and sample
size. One RCT included multiple interventions for a total of 11 unique
interventions. Teaching methods used included instructional tools (n = 9), lecture (n = 6), discussion (n = 3), and demonstration (n = 3). Most interventions (9/11) used multiple teaching methods. The outcome measures reported in the 10 RCTs were cognitive (n = 6), affective (n = 7), and psychomotor (n = 1). Four of the studies measured outcomes in more than one domain.
One
study was able to effectively meet psychomotor learning goals by
teaching proper inhaler technique to patients with asthma and COPD (Numata et al., 2002).
This was done using demonstration and practice. Four of the six studies
reporting improvements included cognitive domain outcomes (Delp & Jones, 1996; Hayes, 1998; Magid et al., 1990; Posner et al., 2004).
All were simple cognitive outcomes such as recall of information and
comprehension measured using knowledge tests. These interventions used
lecture and instructional tools (Delp & Jones, 1996; Magid et al., 1990; Posner et al., 2004) and instructional tools only (Hayes, 1998).
One of the studies that provided an intervention using lecture and
instructional tools provided a home safety kit along with a lecture
about home safety (Posner et al., 2004).
One study included an intervention arm that used discussion and found
no difference with the addition of discussion for simple cognitive
outcomes (Magid et al., 1990).
Two studies failed to meet some or all of the higher-level cognitive
outcomes that required individuals to use information at a later time.
One intervention used lecture, demonstration, and instructional tools;
however, the participants did not meet all of the learning goals (Blank & Smithline, 2002).
The second study measuring higher learning goals had no success in
getting participants to apply the information received. This study used
only instructional tools in the form of an information pamphlet (Ferrari et al., 2005).
Four studies evaluated affective learning goals (Barzargan-Hejazi et al., 2005; Delp & Jones, 1996; Magid et al., 1990; Numata et al., 2002). Two of these studies met simple affective outcomes including satisfaction with instructions and compliance (Delp & Jones, 1996; Numata et al., 2002). These two studies used lecture and instructional tools (Delp & Jones, 1996) and demonstration and practice (Numata et al., 2002).
Two studies also met all higher-level affective outcomes in the form of
change in high-risk behavior using lecture and instructional tools (Magid et al., 1990) and discussion and instructional tools (Barzargan-Hejazi et al., 2005).
In studies where the participants failed to meet some or all of the
learning goals, three measured outcomes in the affective domain using
discussion, demonstration, and practice (Esler et al., 2003), lecture and instructional tools (Richman et al., 2000), and instructional tools only (Ferrari et al., 2005).
In
looking at the entire set of experimental and quasi-experimental
designed intervention studies, the majority (13/19) reported
statistically significant improvements in learning in the intervention
groups (Barzargan-Hejazi et al., 2005; Blank et al., 1998; Clarke et al., 2005; Delp & Jones, 1996; Hayes, 1998; Jolly, 1993; Jolly et al., 1995; Kelso et al., 1995; Lyons et al., 2004; Magid et al., 1990; Numata et al., 2002; O'Malley et al., 2003; Posner et al., 2004; Shrestha et al., 1996). Three studies reported improved outcomes for some of the learning objectives (Berger et al., 1998; Blank & Smithline, 2002; Esler et al., 2003), and three studies reported no improvement in learning (Ferrari et al., 2005; Jolly, 1993; Richman et al., 2000).
Four additional studies included interventions initiated in the ED with follow-up education after discharge (Cote et al., 2001; Guttman et al., 2004; Maiman et al., 1979; Mello et al., 2005).
Three of the four studies reported improved high-level cognitive and
affective outcomes. The interventions included ongoing education
following discharge or continued contact with a healthcare professional (Cote et al., 2001; Guttman et al., 2004; Mello et al., 2005).
The fourth study reported improved high-level cognitive outcomes using
discussion provided by a nurse in the ED who had the condition for which
the participant had received treatment (Maiman et al., 1979).
Supplemental written information was reported as being successful when
adequate verbal instruction was also provided. There was no additional
benefit seen after a 6-week telephone follow-up session (Maiman et al., 1979).
DISCUSSION
Bloom's taxonomy was originally developed to assist in the design and evaluation of educational programs (Redman, 1988). Weston and Cranton (1986)
built on this taxonomy and suggested teaching methods that work
effectively in a variety of scenarios. No articles were found that
explicitly utilized Bloom's taxonomy or Weston and Cranton's framework
for providing patient education in the ED. Using this framework for
health education in the ED may support the use of methods and tools
currently employed and provide insight into alternate methods. However,
some limitations must be considered when using this framework for
patient education. The intent of the framework is to guide teaching in
more traditional classroom settings; thus, there is an implicit
assumption that time and resources are available to educators. This
clearly is one of the major challenges in delivery of patient education
in the ED. Currently, many interventions in the ED use written
instruction. Weston and Cranton note that written materials and handouts
should be considered instructional tools and recommend them as a
supplement to teaching. However, the methods they suggest such as field
study, laboratory instruction, and group projects require personnel and
facilities that may not be possible or appropriate in the ED. Some
methods recommended in the framework were not utilized in the ED. These
include role-playing, games, and simulations. These techniques might be
beneficial, especially when poor literacy is a factor.
When
Bloom's taxonomy was initially created, the authors of the taxonomy
reported that the distinctions between domains were not clear (Redman, 1988).
This is especially true when considering the framework's use with
health education where more operational refinement of the domains would
contribute to better matching of intervention and outcome assessment.
For instance, differentiating between affective domain outcomes and
higher cognitive outcomes remains challenging.
Although
ED staff do not necessarily view their role as supporting secondary
prevention and disease management, the ED is an increasingly important
point of contact for populations known to be frequent ED users, that is,
those with asthma etc. Despite the challenges of providing health
education in the ED, interventions can be effective and this opportunity
to disseminate health information should not be missed.
http://www.nursingcenter.com/library/JournalArticle.asp?Article_ID=774046
http://www.nursingcenter.com/library/JournalArticle.asp?Article_ID=774046
Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου